

To build upon my previous post regarding Evidence-based Strength Training of the Gluteus Medius, I wrote the following article for MedBridge Education…
Pain and Gluteal Strength
The gluteal musculature has been implicated in many different pathologies due to its potential impact on lower extremity biomechanics. During weight bearing, the femur moves about a fixed patella and therefore excessive femoral internal rotation and adduction results in increased contact directed primarily at the lateral facet of the patella1. Just 10° of IR can lead to a substantial decrease in PFJ contract area and a 50% increase in joint stress. Coinciding with these findings, Souza et al.2 found that females with patellofemoral pain syndrome (PFPS) demonstrated greater peak hip internal rotation compared to the control group during running, drop jump, and step down. The PFPS group also demonstrated 14% weaker hip abductor strength and 17% weaker hip extensor strength. Wilson et al3, Noehren et al4, and Nakagawa et al5 found that individuals presenting with PFPS demonstrated increased hip adduction during running, jumping, and single-leg squats. This excess femoral adduction creates an increased valgus force about the knee joint, which in turn causes increased loading of the lateral patellofemoral joint. In addition to patellofemoral pain, a hip etiology or influence has also been implicated in iliotibial band syndrome6, anterior cruciate ligament rupture7, and achilles tendinopathy8. More specifically, impaired gluteus maximus function has been demonstrated in individuals diagnosed with femoroacetabular impingement9.
Gluteal strengthening and Rehabilitation
In support of a gluteal etiology, several studies have found the effectiveness of gluteal strengthening in the treatment of lower extremity disorders. A recent systematic review conducted by Santos and colleagues9 found gluteal strengthening decreased the highest intensity of pain experienced during the previous week, pain when ascending and descending stairs, and pain while squatting or sitting for prolonged periods amongst individuals diagnosed with PFPS. Additionally, with regards to rehabilitation following anterior cruciate ligament reconstruction, the inclusion of hip strengthening appears to improve sagittal plane dynamic balance at three months post-ACLR as compared to traditional rehabilitation10.
EMG Activity and Exercise Goals
According to Reiman et al.11 and Escamilla et al.12, moderate electromyographic activity (EMG) activation (21-40% MVIC) is best used to facilitate endurance and neuromuscular re-education; high activation (41-60+% MVIC) in order to promote strength gains.
From Biomechanics to Exercises
Gluteus Maximus
Origin: Ilium posterior to the posterior gluteal line; dorsal surface of sacrum and coccyx; sacrotuberous ligament
Insertion: Iliotibial tract and gluteal tuberosity
Primary Function: Extends thigh and assists in hip abduction and external rotation; steadies thigh and assists in rising from sitting position
Among introductory exercises, the gluteus maximus achieves the highest EMG levels during:
- Front-plank with Hip Extension
- Gluteal Squeeze
- Side-plank with Hip Abduction
- Quadruped with Contralateral Arm/Leg Lift
- Uni-lateral Bridge

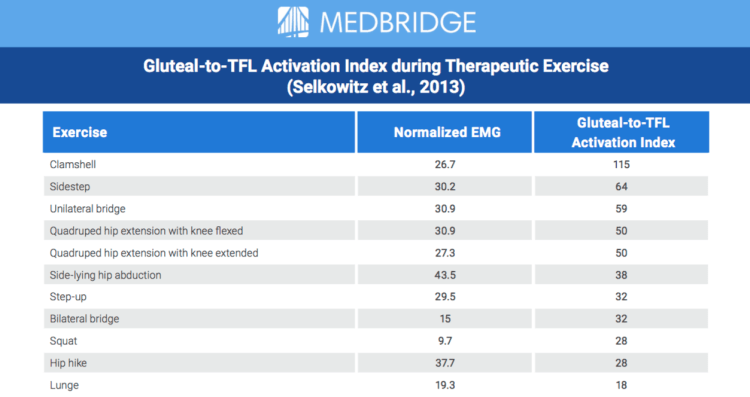
Additionally, you must consider the interaction of other muscles acting with or against the gluteus maximus when determining exercise prescription. It has been proposed that individuals who demonstrate excess femoral internal rotation during functional tasks may be relying too heavily on the tensor fasciae latae to control their pelvis in the presence of weak or inhibited gluteus medius musculature.
Selkowitz and colleagues determined that the following exercises achieved the best Gluteal to Tensor Fasciae Latae Activation Ratio:
- Clamshell
- Side-step with resistance band
- Single-leg bridge
- Quadruped hip extension with knee extended
- Quadruped hip extension with knee flexed
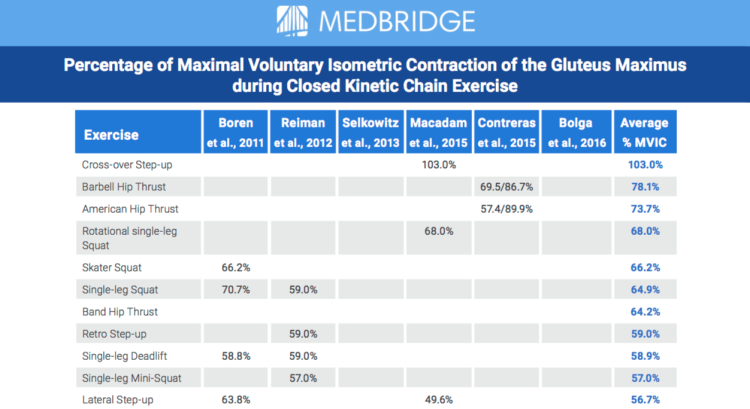
Finally, when progressing your patient towards more functional closed kinetic chain and sport/activity-specific exercises, the following exercises achieve the highest gluteus medius activation:
- Cross-over Step-up
- Hip Thrust Variations (Barbell, Band, American)
- Rotational Single-Leg Squat
- Skater Squat
- Single-Leg Squat
Exercise prescription is a multi-faceted decision, which is driven by the individual patient’s goals, functional limitations, and the evidence supporting the treatment of these factors. Using EMG studies to drive the selection of exercise is highly valuable, especially during the early stages of rehabilitation or when attempting to isolate individual muscles and/or groups of muscles. However, there are limitations when comparing different studies due to methodological differences (the type of EMG, patient population, data analysis, etc.). Additionally, due to the cost and time to conduct these studies, there are thousands of exercises that have not been evaluated in the literature. In light of this information, these studies should be used to guide your decision making, it should not override your clinical expertise when accompanied by biological plausibility.
Continued reading…




